One of the largest challenges for cannabis research is the standardization of cannabis dose. In this article of Evidence in Context: Much Ado about Dosing, the Consortium assesses the needs and challenges of defining a standardized cannabis unit.
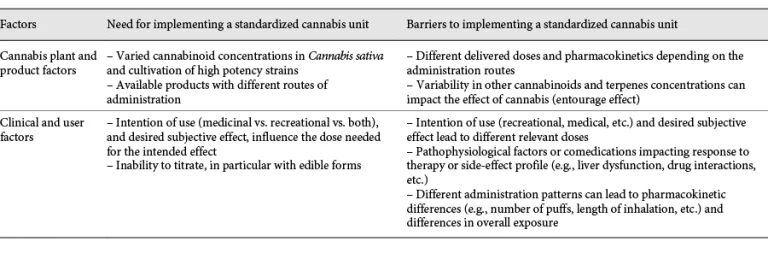
Needs and barriers for the implementation of a standardized cannabis unit
Factors:
Need for implementing a standardized cannabis unit
Barriers to implementing a standardized cannabis unit
Cannabis plant and product factors:
Need for implementing a standardized cannabis unit:
Varied cannabinoid concentrations in Cannabis sativa and cultivation of high potency strains
Available products with different routes of administration
Barriers to implementing a standardized cannabis unit:
Different delivered doses and pharmacokinetics depending on the administration routes
Variability in other cannabinoids and terpenes concentrations can impact the effect of cannabis (entourage effect)
Clinical and user factors:
Need for implementing a standardized cannabis unit:
Intention of use (medicinal vs. recreational vs. both), and desired subjective effect, influence the dose needed for the intended effect
Inability to titrate, in particular with edible forms
Barriers to implementing a standardized cannabis unit:
Intention of use (recreational, medical, etc.) and desired subjective effect lead to different relevant doses
Pathophysiological factors or comedications impacting response to therapy or side-effect profile (e.g., liver dysfunction, drug interactions, etc.)
Different administration patterns can lead to pharmacokinetic differences (e.g., number of puffs, length of inhalation, etc.) and differences in overall exposure
A recent review of medical cannabis clinical research in the USA showed significant variability in the dose, route of administration, and THC/CBD content of cannabis products studied. Such variability limits the ability to compare and summarize study findings as well as the ability to formulate recommendations for use in clinical practice.
Researchers have proposed a “Standard THC Unit” of 5 mg based on the premise that THC is the principal constituent responsible for the psychoactive effects of cannabis
There are some strengths and limitations to the implementation of the “Standard THC Unit”, including:
Strengths
Guide clinicians and patients in initiating, maintaining, and adjusting cannabis therapy
Potentially improve identification and management of problematic cannabis use
Improve patient education and clarifying informational materials
Limitations
Complex clinical and pharmacological nature of cannabis (CBD vs. THC)
Multiple varieties of cannabis plant and the routes of administration
User factors (i.e., medical use vs. non-medical use, drug-drug interactions, etc.)
While there is a consensus on the importance of a standardized cannabis unit, it is unlikely that a “one size fit all” definition will capture all the needs of cannabis use.
As more standardized cannabis units are proposed, the focus should include considerations for the increasing use of medical cannabis and cannabinoids, the role of CBD, and the administration routes.